


顴骨下顎骨眉棱骨削骨
削骨:
顴骨、下顎骨、眉棱骨
在台灣,一般削骨跟拉皮通常是分開進行手術,因為兩種手術各自時間都很長,而且大部分的醫師在進行手術時,其單一手術都有不等的出血量及水腫,另外削骨要有口內切口,拉皮又要有外面皮膚的切口,因為有這些考慮,這就是所有的醫師會建議分開手術,不要同時進行
單純削骨,術後讓有些人可能會覺得效果不如預期,而且常常會造成術後的臉部皮膚鬆垮下垂
對於寬臉圓臉的人,如果只有單純拉皮,沒有處理骨頭,結果通常會不如預期,因為臉型不漂亮,沒有媽媽變回年輕小姐的感覺
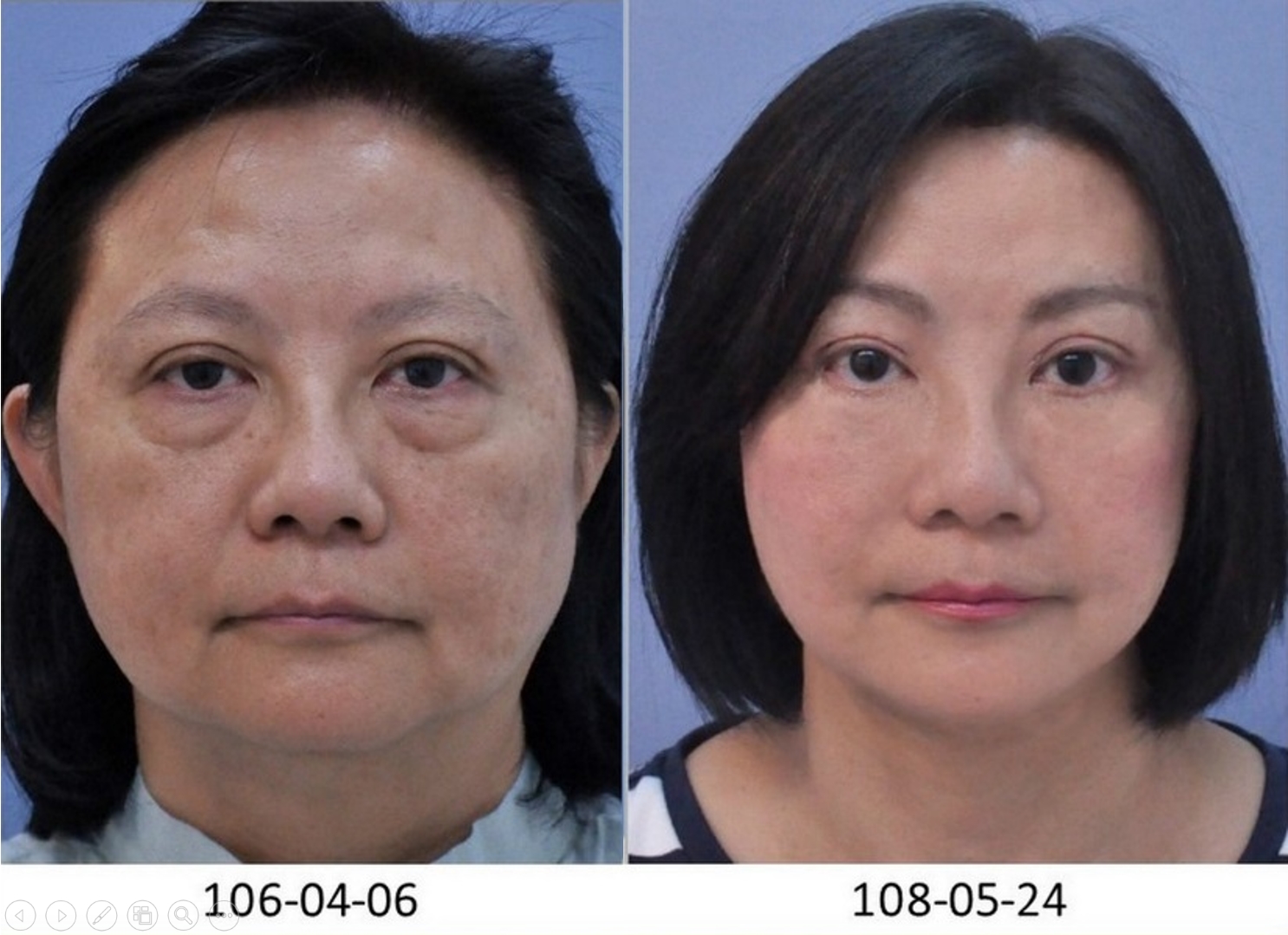
亞洲人常常比西洋人更有明顯的眼尾下垂,三角眼,找很多整形外科做雙眼皮手術矯正,卻不見其效果,其主要原因是因為先天突起下壓的眉棱骨導致,因此在額頭拉皮手術中,搭配磨掉突起下壓的眉棱骨,就可以改善眼尾下垂、三角眼,使得拉皮手術效果更好,改變眼型找回迷人的電眼
削顴骨案例照:


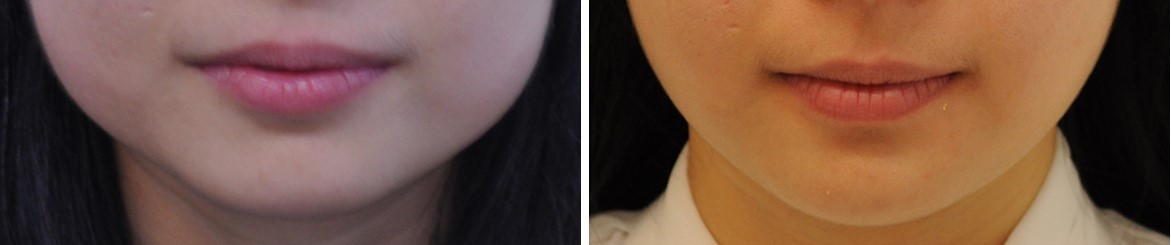
下顎骨削骨案例照 :
.jpg)
.jpg)

.jpg)
.jpg)
.jpg)

.jpg)
案例已經過當事人同意刊登露出,並簽署同意公開授權書。僅作為手術醫療資訊之介紹分享。
本文術前術後案例照,為手術醫療資訊介紹分享,其治療效果會因個人 體質 與 術後保養 而有異。
諾美整形外科診所提醒您,任何手術與醫療處置均有潛在風險,並非每個人都適合,本文 內容僅供參考,實際須由醫師當面與您進行評估及溝通而定。
Facelift alone for round face patients often yielded an unideal cosmetic outcome, therefore, according to previous experience, it is more desirable that surgeons change bony structure ahead of performing facelifts in those patients with a protruding mala or widened mandible[1, 2, 4]. Reduction malarplasty alone for wide face patients has found an incidence of soft-tissue sagging and cheek descent postoperatively, and in our practice, these patients usually seek for further facelift 6 months after previous bone surgery.
Aging in the middle and low face area is associated not only with soft-tissue drooping but also with the widening of zygoma and mandible, and descent of the malar area[5, 6]. These all provide insufficient facial projection and result in an old-looking and unattractive face. That is why an effective facial rejuvenation cannot be achieved by simply a facelift, especially in Asians with a wide zygoma projection or prominent mandibular angle.
Besides, compared to Caucasian, Asians tend to have congenital lateral hooding of upper eyelid related to downward eyebrow ridge, contributed to an aging and less attractive facial appearance (Fig. 1), and in those severe cases (Fig. 11), the shaving of supraorbital ridges should be applied. Some of these cases were found with no improvement after mistakenly operated with several times of blepharoplasty under illusion to improve lateral hooding.
Facelift and bone contouring are two time-consuming surgeries with different lengthy incisions (external facelift incision v.s. intra-oral bony reduction incision), blood loss in bone reshaping, enhanced swelling, are often performed as two separate procedures.
Few articles mentioned simultaneous facelift and facial bone contouring before[1, 3]. For zygoma reduction and midface lift, Baek and Lee[1], in 2009, demonstrated malar repositioning through bicoronal approach, dissection under the temporoparietal fascia, osteotomy with bone fixation and a simultaneous periosteal midface lift and forehead lift. In 2016, Zou and Wang[3] further exhibited multiple-incision simultaneous intra-oral reduction malarplasty with transverse temporal incision cheek-lift, and described Baek’s method of having the advantage of wider operative field and easier conduction of a forehead lift, but overly traumatic for those who did not require a forehead lift and had the shortcomings of longer operative time and longer scalp scar. In author's opinion, Baek’s method fails in complete exposure of zygoma, hence results in the inconvenience of hemostasis and precise bone fixation. Zou and Wang’s method of intraoral and external facelift incisions had sustaining problems of long operative time, incomplete vision of the surgical field, increased blood loss and postoperative swelling, intraoral infection, as well as oral intake discomfort.
For solitary zygoma reduction or mandible angle resection, all described operative methods are performed through an intraoral approach[7, 8] because it can avoid the external scar. However, the intraoral-only approach also has some complications because of its limited operative visibility and restricted movement of the oscillating saw, subcondyle fracture, massive hemorrhage and bone asymmetry in particular[9]. Lei and Wang[10] therefore presented a modified intraoral and external approach for the prominent mandibular angle, with the usage of a reciprocating saw through an extraoral incision created in the auriculocephalic sulcus behind the earlobe. However, from author’s point of view, when combined with facelift, the facelift approach can be used with no other access when the supraorbital ridge, zygoma or mandible require contouring. In our practice, supraorbital ridge correction can be performed through forehead coronal incision, whereas zygoma reduction can be performed using middle facelift incision, and mandibular angle resection can be performed using lower facelift incision with extension approximate 3 cm at retroauricular hairline.
By our method, owing to the extensive subcutaneous dissection in facelift, the surgeon can visualize targeted bone directly, protect nearby vessels and nerves, and the difficulty in blood management is lessened. The bone reduction is thus more accurate and safer with shortened operation time and minimal blood loss of less than 30 ml. Hirohi and Yoshimura[11] reported that in their 519 cases of intraoral approach mandibular angle osteotomy, the average operation time for combination of en-bloc mandibular corpus-angle ostectomy and corticectomy was 95 minutes, ranged from 76 to 164 minutes. Yoon, E.S., et al.[12] analyzed the data from 33 surgeons in South Korea conducting summing up to 1251 intraoral approach mandibular angle osteotomy. For bilateral angle osteotomy, it took less than 1 hour in 9% of all cases, about 1 to 2 hours in 36%, and about 2 to 3 hours in 45%. Comparatively, the average operation time of our method for external bilateral mandibular angle resection is about 1 hour, which is relatively shorter than other procedures.
The major advantages of the facelift incision are direct vision, time-saving, precise contouring of the selected bones, especially in wide-jaw patients with prominent posteroinferior projection. However, this procedure was rarely used may because of the following disadvantages. First, the surgeon must be well-experienced in both facial bone reduction and facelift surgeries. Secondly, the anatomic dissection of periorbital and mandible angle area must be familiar to the operator in order to (Fig. ). These all require a long learning curve and practicing experiences.
With regard to facelift surgery, numerous variations in techniques have been described. Though, it remains impossible to define which techniques are best given subjectivity, differences in aesthetic judgement, patient differences, and small sample size[13].
Dr. Rohrich[14] in 2016 represented that early in his experience, the extended SMAS dissection was performed, however, the deep plane technique has been abandoned for an SMAS plication or SMASectomy. In his hands, the latter technique provides similar results without the extensive dissection of the SMAS. We agreed and carried out this concept for years. It can avoid the threats of facial nerve damage, meanwhile, demand less dissection time. That’s why we can not only save time in performing facelift, but also perform in a safer way, on the other hand, yield good cosmetic outcome.
As a consequence, performing facelift with multiple bone contouring in single incision is a logical approach for those patients who complained of downward eyebrow ridge, prominent zygoma or wide mandible, with or without aging face. Our experience with this technique suggests that this procedure can be performed safely with satisfactory results.
填寫表單
歡迎填寫表單,與我們聯繫或撥打諮詢專線 02-27117999
私人資料受個人隱私保密原則保護,絕不對外洩露,敬請安心!
私人資料受個人隱私保密原則保護,絕不對外洩露,敬請安心!